

Dr. Kevin McCairn and patient Ken Evans joined me to discuss a promising intervention for severe COVID-19 vaccine injuries. Conducted from Japan, where McCairn and colleagues treat patients, the conversation highlights the debilitating effects of vaccine-induced amyloid formation and a novel therapeutic approach offering dramatic recoveries.
McCairn, who has treated approximately 25 patients, describes vaccine injuries linked to abnormal amyloid and mis-folded proteins, often triggered by spike protein. These cause widespread microclots, autoimmune responses, brain fog, extreme fatigue, heart irregularities, neuropathy, and organ damage. Many patients arrive after years of misdiagnosis and ineffective treatments, having spent hundreds of thousands of dollars.
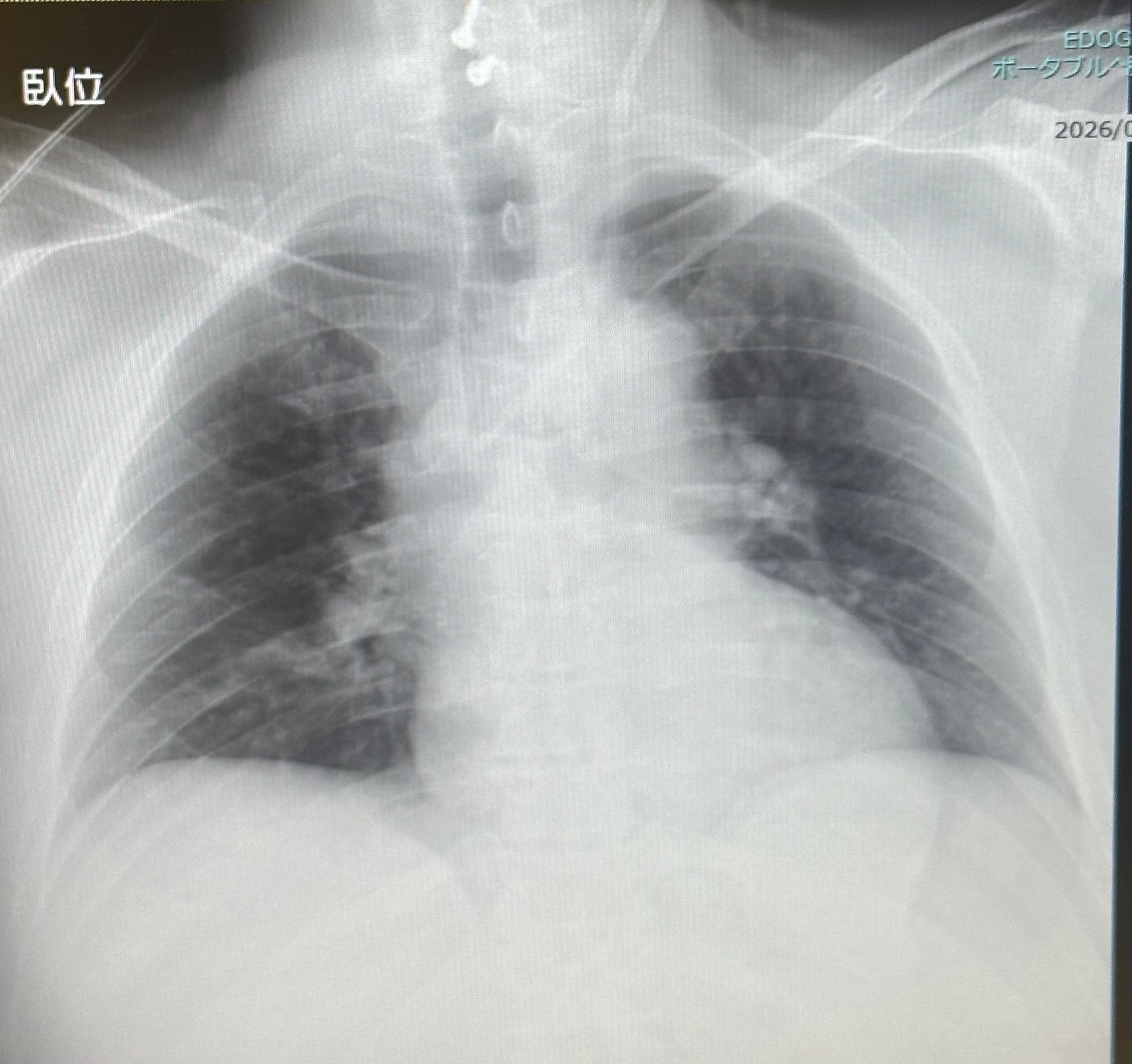
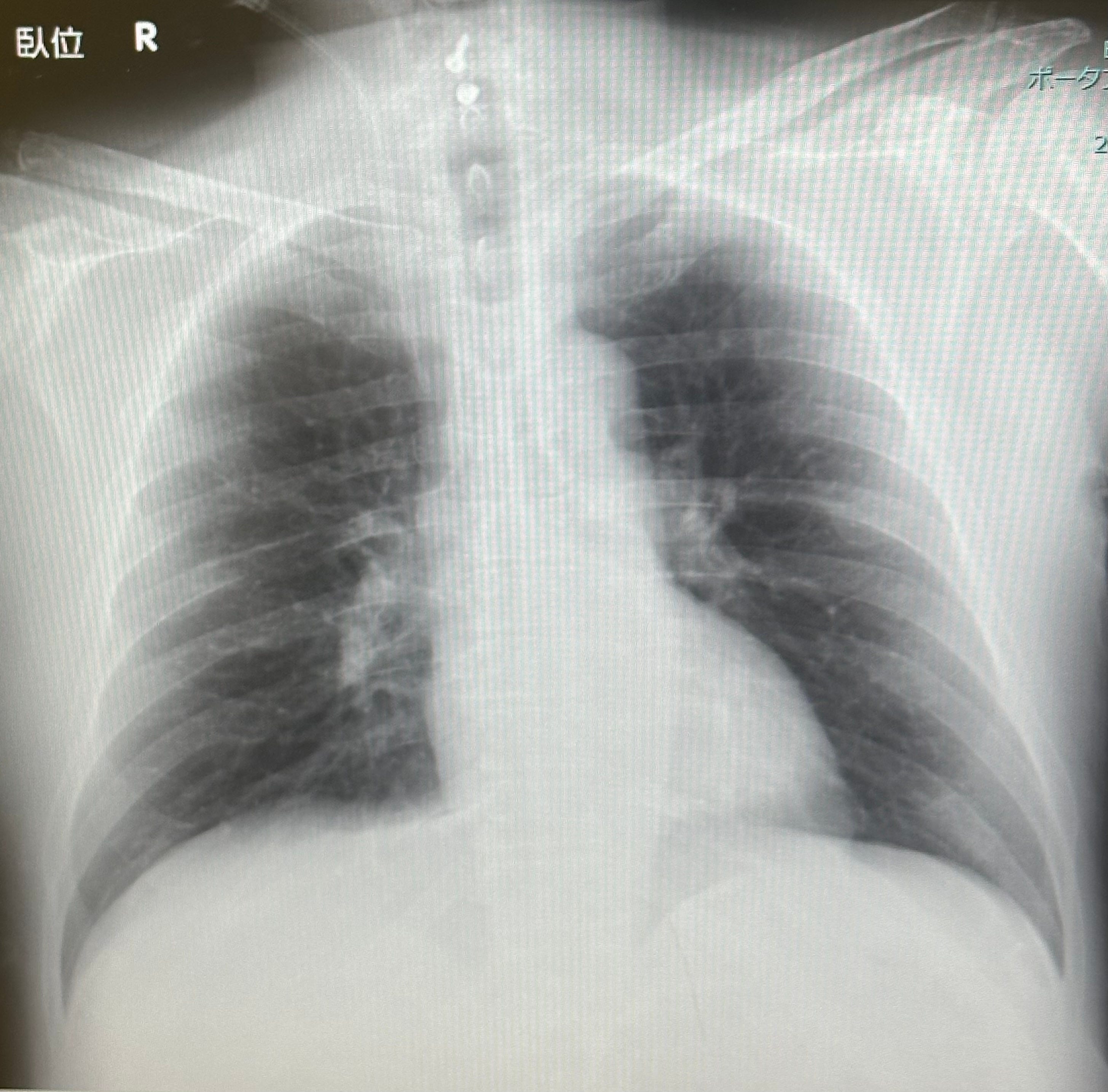
Evans, a former rugby player from Houston, exemplifies this struggle. Vaccinated in March 2021, he rapidly developed symptoms: skyrocketing spike antibodies (over 18,000), low B cells, liver dysfunction, endocrine chaos, autoimmune encephalitis, and malignant pericarditis visible on X-rays as a large inflamed sac around the heart. Conventional tests (cardiac MRI, stress tests) appeared normal, and doctors dismissed vaccine causation, sometimes bordering on malpractice. Thyroid removal worsened his condition. He endured ER visits with heart rates spiking to 190 bpm, fainting, blood in multiple sites, and profound brain fog that stripped him of emotion and clarity. “I was dying,” Evans recalls. “I couldn’t get out of bed.”
The Japan protocol involves jugular-vein dual filtration apheresis using specialized canisters to remove autoantibodies, amyloids, and misfolded proteins directly from cerebral outflow, combined with stem cell growth factors (SGF) derived from dental pulp to promote regeneration and inhibit further clotting. Unlike peripheral vein methods, this targets neurovascular injury.
Evans underwent four weeks of treatment. After the first filtration, his cognitive clarity returned. Post-second session, the pressure in his heart and panic lifted. X-rays three weeks later showed near-complete resolution of pericarditis. Spike antibodies dropped 25%, and he regained 85% function—able to laugh, parent, and live normally, though managing residual Hashimoto’s. “I have my life back,” he says.
Chest X-Rays of Ken Evans before and after treatment:
Many others report rapid relief from brain fog and fatigue, with spectacular turnarounds even in severe cases. Nurse Lindsay, previously housebound for years, is now able to run. Recovery is slower with extensive brain damage but generally positive.
Challenges remain. Treatment costs are high, unavailable in the U.S. due to regulatory hurdles, and patients often exhaust resources first. McCairn notes emerging hydrogel-like plasma changes in samples, raising concerns about broader contamination risks. He stresses autoantibodies and molecular mimicry drive much pathology beyond persistent spike. While not a universal cure, the intervention achieves clinical significance for many.
Evans’ story underscores medical gaslighting yet offers hope. As advocates push for U.S. access and recognition, this protocol demonstrates that targeted removal of pathological proteins paired with regenerative support can reverse what seemed irreversible damage. For countless injured individuals, it represents not just treatment, but restored humanity.
If you are interested in having your blood tested for amyloid, go to Synpatek Labs for further instructions.
